Follow-Up Study Compares Family Food Culture in Three Countries
Learning Life’s Director, Paul Lachelier, plus medical student Anudeep Alberts, Dr. Melissa See and Dr. Kim Bullock of the Georgetown University School of Medicine (GUSM) co-presented a joint study of the food culture of lower-income families in three countries on Monday this week at the Health Literacy Annual Research Conference (HARC) in Bethesda, Maryland.
The cross-national study is a follow-up to research conducted by Drs. Lachelier and See earlier this year. The two studies are intended to better understand the food culture (i.e., shopping, cooking and eating practices, and the meanings attached to those practices) of selected families participating in Learning Life’s Family Diplomacy Initiative (FDI) in Washington DC, San Salvador, El Salvador, and Dakar, Senegal, with an eye to improving their health outcomes in the long-term.
Since Fall 2017, Learning Life has been collaborating with GUSM’s Community Health Division on international research and programming, including our food culture project, and more recently our project-supporting family “cook, eat and learn sessions” or CELS. Starting with that food culture project launched this year, Learning Life is grounding its FDI family-to-family projects in health. As Lachelier explains, “the vigor and happiness of individuals, families, communities, societies, indeed the entire world depends on good health. In turn, human health is also impacted by a myriad of factors, from the local food supply to global climate change. This makes health a vital, rich and flexible way for our families to learn about the wider world.” (Click here for more about FDI’s turn to health.)
Since May, GUSM medical student, Anudeep Alberts, among other things worked diligently with Lachelier on the data collection then writing for this research poster. “We look forward to more collaboration with Learning Life on its innovative Citizen Diplomacy Initiative,” said Bullock, who directs GUSM’s Community Health Division. The poster is featured here, and below is the poster’s full text in larger print for readability. For a PDF copy of the poster, contact us at email@learninglife.info.
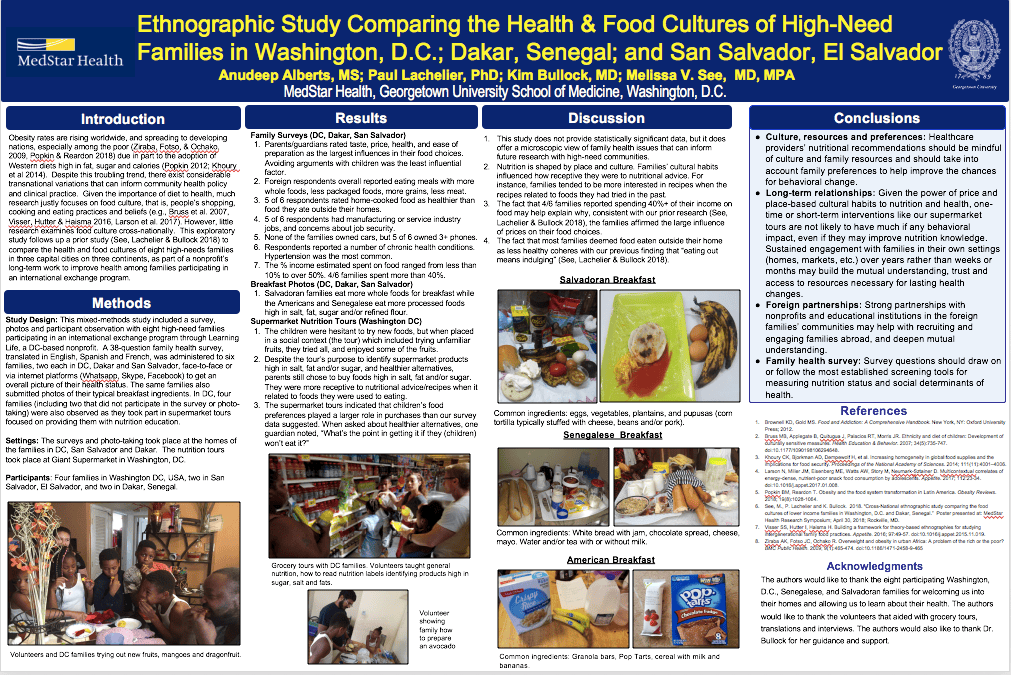
Ethnographic Study Comparing the Health & Food Cultures of High-Need Families in Three Countries
Introduction
Obesity rates are rising worldwide, and spreading to developing nations, especially among the poor (Ziraba, Fotso, & Ochako, 2009, Popkin & Reardon 2018) due in part to the adoption of Western diets high in fat, sugar and calories (Popkin 2012; Khoury et al 2014). Despite this troubling trend, there exist considerable transnational variations that can inform community health policy and clinical practice. Given the importance of diet to health, much research justly focuses on food culture, that is, people’s shopping, cooking and eating practices and beliefs (e.g., Bruss et al. 2007, Visser, Hutter & Haisma 2016, Larson et al. 2017). However, little research examines food culture cross-nationally. This exploratory study follows up a prior study (See, Lachelier & Bullock 2018) to compare the health and food cultures of eight high-needs families in three capital cities on three continents, as part of a nonprofit’s long-term work to improve health among families participating in an international exchange program.
Methods
Study Design: This mixed-methods study included a survey, photos and participant observation with eight high-need families participating in an international exchange program through Learning Life, a DC-based nonprofit. A 38-question family health survey, translated in English, Spanish and French, was administered to six families, two each in DC, Dakar and San Salvador, face-to-face or via internet platforms (Whatsapp, Skype, Facebook) to get an overall picture of their health status. The same families also submitted photos of their typical breakfast ingredients. In DC, four families (including two that did not participate in the survey or photo-taking) were also observed as they took part in supermarket tours focused on providing them with nutrition education.
Settings: The surveys and photo-taking took place at the homes of the families in DC, San Salvador and Dakar. The nutrition tours took place at Giant Supermarket in Washington, DC.
Participants: Four families in Washington DC, USA, two in San Salvador, El Salvador, and two in Dakar, Senegal.
Results
Family Surveys (DC, Dakar, San Salvador)
1.Parents/guardians rated taste, price, health, and ease of preparation as the largest influences in their food choices. Avoiding arguments with children was the least influential factor.
2.Foreign respondents overall reported eating meals with more whole foods, less packaged foods, more grains, less meat.
3.5 of 6 respondents rated home-cooked food as healthier than food they ate outside their homes.
4.5 of 6 respondents had manufacturing or service industry jobs, and concerns about job security.
5.None of the families owned cars, but 5 of 6 owned 3+ phones.
6.Respondents reported a number of chronic health conditions. Hypertension was the most common.
7.The % income estimated spent on food ranged from less than 10% to over 50%. 4/6 families spent more than 40%.
Breakfast Photos (DC, Dakar, San Salvador)
1.Salvadoran families eat more whole foods for breakfast while the Americans and Senegalese eat more processed foods high in salt, fat, sugar and/or refined flour.
Supermarket Nutrition Tours (Washington DC)
1.The children were hesitant to try new foods, but when placed in a social context (the tour) which included trying unfamiliar fruits, they tried all, and enjoyed some of the fruits.
2.Despite the tour’s purpose to identify supermarket products high in salt, fat and/or sugar, and healthier alternatives, parents still chose to buy foods high in salt, fat and/or sugar. They were more receptive to nutritional advice/recipes when it related to foods they were used to eating.
3.The supermarket tours indicated that children’s food preferences played a larger role in purchases than our survey data suggested. When asked about healthier alternatives, one guardian noted, “What’s the point in getting it if they (children) won’t eat it?”
Discussion
1.This study does not provide statistically significant data, but it does offer a microscopic view of family health issues that can inform future research with high-need communities.
2.Nutrition is shaped by place and culture. Families’ cultural habits influenced how receptive they were to nutritional advice. For instance, families tended to be more interested in recipes when the recipes related to foods they had tried in the past.
3.The fact that 4/6 families reported spending 40%+ of their income on food may help explain why, consistent with our prior research (See, Lachelier & Bullock 2018), the families affirmed the large influence of prices on their food choices.
4.The fact that most families deemed food eaten outside their home as less healthy coheres with our previous finding that “eating out means indulging” (See, Lachelier & Bullock 2018).
Conclusions
Culture, resources and preferences: Healthcare providers’ nutritional recommendations should be mindful of culture and family resources and should take into account family preferences to help improve the chances for behavioral change.
Long-term relationships: Given the power of price and place-based cultural habits to nutrition and health, one-time or short-term interventions like our supermarket tours are not likely to have much if any behavioral impact, even if they may improve nutrition knowledge. Sustained engagement with families in their own settings (homes, markets, etc.) over years rather than weeks or months may build the mutual understanding, trust and access to resources necessary for lasting health changes.
Foreign partnerships: Strong partnerships with nonprofits and educational institutions in the foreign families’ communities may help with recruiting and engaging families abroad, and deepen mutual understanding.
Family health survey: Survey questions should draw on or follow the most established screening tools for measuring nutrition status and social determinants of health.
References
1.Brownell KD, Gold MS. Food and Addiction: A Comprehensive Handbook. New York, NY: Oxford University Press; 2012.
2.Bruss MB, Applegate B, Quitugua J, Palacios RT, Morris JR. Ethnicity and diet of children: Development of culturally sensitive measures. Health Education & Behavior. 2007; 34(5):735-747. doi:10.1177/1090198106294648.
3.Khoury CK, Bjorkman AD, Dempewolf H, et al. Increasing homogeneity in global food supplies and the implications for food security. Proceedings of the National Academy of Sciences. 2014; 111(11):4001–4006.
4.Larson N, Miller JM, Eisenberg ME, Watts AW, Story M, Neumark-Sztainer D. Multicontextual correlates of energy-dense, nutrient-poor snack food consumption by adolescents. Appetite. 2017; 112:23-34. doi:10.1016/j.appet.2017.01.008.
5.Popkin BM, Reardon T. Obesity and the food system transformation in Latin America. Obesity Reviews. 2018; 19(8):1028-1064.
6.See, M., P. Lachelier and K. Bullock. 2018. “Cross-National ethnographic study comparing the food cultures of lower income families in Washington, D.C. and Dakar, Senegal.” Poster presented at: MedStar Health Research Symposium; April 30, 2018; Rockville, MD.
7.Visser SS, Hutter I, Haisma H. Building a framework for theory-based ethnographies for studying intergenerational family food practices. Appetite. 2016; 97:49-57. doi:10.1016/j.appet.2015.11.019.
8.Ziraba AK, Fotso JC, Ochako R. Overweight and obesity in urban Africa: A problem of the rich or the poor? BMC Public Health. 2009; 9(1):465-474. doi:10.1186/1471-2458-9-465.
Acknowledgments
The authors would like to thank the eight participating Washington, D.C., Senegalese, and Salvadoran families for welcoming us into their homes and allowing us to learn about their health. The authors would like to thank the volunteers that aided with grocery tours, translations and interviews. The authors would also like to thank Dr. Bullock for her guidance and support.
Pilot Global Storytelling Challenge Launches
Today, six DC middle school students and two Learning Life teachers met for the first time to launch an experiment in Washington DC: a global storytelling challenge.
Since Learning Life started its Citizen Diplomacy Initiative (CDI) a little more than two years ago, in August 2016, we have recruited some of our CDI families from schools in Washington DC, but we have not established a working relationship with any school, until now. Starting today, two volunteer Learning Life teachers, Nichole Hutchins and Rujjares Hans, both Master’s students in the International Education Program at George Washington University, are leading six students at the Saint Thomas More Catholic Academy (STM), with the assistance of STM Social Studies teacher, Randall Carter, in a challenge focused on telling stories about health from an international perspective.
“Countless pressing public issues are health issues, including bullying, depression, loneliness, drug abuse, crime, hunger, obesity, diabetes, homelessness, unemployment, income and wealth inequality, human trafficking, communicable diseases, terrorism, war, pollution, and climate change. Good health is fundamentally important, yet research indicates that lower-income families suffer disproportionately from health problems. Storytelling is a widely useful, resume-building skill any person can develop, regardless of their material resources, and an effective way to learn about any topic, including health. However, there are relatively few opportunities for lower-income youth, including many STM students, to develop their storytelling skill, especially in an international context,” explained Learning Life’s Founder and Director, Paul Lachelier.
Thus, from October 22 to December 10, 2018, Nichole and Rujjares will meet with their elementary school students for 1.5 hours weekly to learn, plan and ultimately perform before a live audience two compelling stories about an international issue that affects health. The group will form two teams, each composed of three students and one teacher. Each team will develop its own engaging health story, choosing their international issue and story form (dance, song, poetry, miming, painting, writing, etc., or some combination thereof). Each story, told in 5-10 minutes, must connect the local with the global, either by comparing or connecting two stories in different parts of the world, or by connecting a local story to a global phenomenon or trend. In their last meeting on December 10, the two student teams will perform their stories and be judged by a panel of storytelling experts in front of a live audience of students, teachers and staff.
When all is said and done, the challenge should give the student storytellers valuable experience in developing and performing a story, and a deeper understanding of world health issues. Learning Life will survey the students at the start and end of the challenge to gauge its impact on the students’ attitudes and knowledge about the world. If this pilot storytelling challenge proves successful, we aim to do a second challenge in the spring with more STM students with an eye toward expanding the competition to more schools in Washington DC and in other cities where Learning Life works abroad in the coming years.
Introducing “Cook, Eat & Learn Sessions” (CELS)
This fall and winter, six Georgetown University medical students will meet with lower-income Washington DC families participating in Learning Life’s Citizen Diplomacy Initiative (CDI) to conduct what we call “cook, eat and learn sessions” or CELS. The CELS will support the American families engaged in our CDI food culture project in learning about nutrition and differences in shopping, cooking and eating practices internationally.
Each year, first-year Georgetown University medical students are required to complete a community-based learning (CBL) course. Through the course, students gain community-based experience about the “social determinants of health” — socio-economic factors like employment, housing, transportation, education, and access to supermarkets — as they assist community organizations by educating and/or conducting basic health exams with lower-income DC residents. This fall is the first time students in the CBL course will be volunteering with Learning Life.
If all goes according to plan, the medical students, working in pairs — Claire and Matt, Nikita and George, Dahlia and Amna — will meet with five CDI families, one at a time, at their respective homes to (1) cook a meal that is healthy, cheap, tasty, foreign and easy to make, and (2) during the meal make a Powerpoint presentation about their experience of foreign food cultures while traveling or living abroad. The students (featured in the above photo along with their faculty lead, Dr. Kim Bullock, and Learning Life Director, Paul Lachelier) all elected into conducting the CELS given their interest in food, nutrition and/or travel.
“DC, like so many cities worldwide, is highly segregated by class and race. People of different socio-economic status may cross paths as strangers or at best polite acquaintances on the street, in stores, or at work, but rarely do they interact meaningfully, let alone cook and eat together. CELS are intended to bridge that socio-economic divide via something all humans do — food — while giving lower-income families the opportunity to learn a little about nutrition, healthy cooking, and food cultures in other countries,” explains Learning Life Director, Paul Lachelier.
“Our students are excited to participate in the CELS. I anticipate they will learn just as much from the experience as the families will,” said Dr. Bullock, who is also a practicing doctor, professor, and Director of the Community Health Division at the Georgetown University School of Medicine.
CELS follow on several supermarket nutrition tours Learning Life volunteers conducted with some of our American families this summer to teach them about nutrition labeling and healthier food shopping, and to try new fruits, like kiwi, mango, pomegranates and dragon fruit (see the above photo).
Toward Good Health, Local to Global
Good health is vital. The less healthy one is, the less one is able to perform as a private individual in school, work and family, let alone as a public citizen in community and society. The vigor and happiness of individuals, families, communities, societies, indeed the entire world, thus depends on good health. In turn, human health is also impacted by a myriad of factors, from the local food supply to global climate change. These are two major reasons why Learning Life has begun orienting our programming toward health.
Countless pressing public issues are health issues, including bullying, child abuse, domestic violence, depression, loneliness, drug abuse, drunk driving, gun violence, hunger, obesity, diabetes, heart disease, homelessness, poverty, unemployment, income and wealth inequality, human trafficking, communicable diseases ranging from common cold viruses to deadly Ebola, terrorism, war, pollution, and climate change. As this long yet far from complete list demonstrates, health issues run from violence at home, or bullying in one’s school or neighborhood, to international phenomena like human trafficking, terrorism and climate change. Furthermore, many of these health issues are interconnected and happen in many localities yet they are shaped by big, complicated histories and institutional actors — religious faiths, multinational businesses, national governments, international governmental bodies — whose powerful actions are often invisible and incomprehensible to all but a few trained and paid specialists. Thus, human health is affected by so many issues local to global yet the connections and causes of those issues are dauntingly complex.
Faced with such complex health problems, it is tempting to ignore them. But ironically, the less one knows, the more one is at risk for avoidable health problems (e.g., those less educated are more likely to smoke, take drugs, overeat, etc.) while other health threats, like drunk driving, inequality, and climate change, one can ignore but cannot avoid entirely, if at all. Those who are resource-poor are the least able to avoid many public problems that have health impacts. So, we can either put our heads in the sand, or take action, and Learning Life aims to take action.
Accordingly, in fall 2017, Learning Life began collaborating with the Georgetown University School of Medicine’s (GUSM) Community Health Division. That collaboration helped propel Learning Life’s research this year comparing the health and food cultures of our CDI (Citizen Diplomacy Initiative) families in Washington DC, San Salvador, El Salvador, and Dakar, Senegal (click here for the first study, with further research results coming soon), and our larger family food culture project. Food clearly impacts health, and has the educational advantage of being a universal, daily preoccupation of interest to most people. Food culture — which we define as a group’s food shopping, cooking and eating habits and beliefs — also varies substantially cross-nationally, and can be shaped to advance health and learning about the world. Hence, food culture seems a fitting focus for our project work between CDI families in different countries.
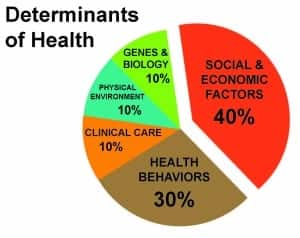
The GUSM Community Health Division, under the leadership of Dr. Kim Bullock, welcomes partnerships with community organizations to help improve community health education while giving Georgetown medical students experience in what the medical profession commonly calls “the social determinants of health” (SDHs). A pie chart (University of North Carolina-Charlotte 2018) often employed to provide U.S. medical students and health professionals with perspective on the determinants of health gives a sense of the importance of SDHs:
As the chart shows, SDHs have the largest impact on people’s health, surpassing individuals’ own actions (diet, exercise, smoking, drug-taking, etc.), and much surpassing a person’s genetics, environment, or medical care resources. The second chart below (Kaiser Family Foundation 2018) unpacks the SDH term, giving a sense of the wide range of SDHs, and hence why these factors, together, matter so much to human health:
The chart underscores that while good or bad health is experienced individually, it is shaped by a range of social factors, some of which, like literacy and language, too many people may not realize are linked to their health. As our world grows more interconnected economically, socially and politically, many of these SDHs are shaped more and more by international forces like trade, immigration and climate change. It thus behooves health educators to frame learning about health in local to global terms.
In the shorter term, the shared challenge of Learning Life and GUSM’s Community Health Division is to improve CDI families’ understanding of health, including nutrition and SDHs, and food culture, wherever they are in the world. In the longer term, we hope to improve the health outcomes of our families worldwide. Much that is good on this Earth takes time and patient work to happen. That is why we are in this for the long haul.
Kaiser Family Foundation. “Beyond Health Care: The Role of Social Determinants in Promoting Health and Health Equity.” Chart retrieved from https://www.kff.org/disparities-policy/issue-brief/beyond-health-care-the-role-of-social-determinants-in-promoting-health-and-health-equity/ on 9/7/18.
University of North Carolina-Charlotte. “ARCHES Mission & Goals.” Chart retrieved from https://arches.uncc.edu/mission-goals on 9/7/18.

 The cross-national study is a follow-up to research conducted by Drs. Lachelier and See earlier this year. The two studies are intended to better understand the food culture (i.e., shopping, cooking and eating practices, and the meanings attached to those practices) of selected families participating in Learning Life’s Family Diplomacy Initiative (FDI) in Washington DC, San Salvador, El Salvador, and Dakar, Senegal, with an eye to improving their health outcomes in the long-term.
The cross-national study is a follow-up to research conducted by Drs. Lachelier and See earlier this year. The two studies are intended to better understand the food culture (i.e., shopping, cooking and eating practices, and the meanings attached to those practices) of selected families participating in Learning Life’s Family Diplomacy Initiative (FDI) in Washington DC, San Salvador, El Salvador, and Dakar, Senegal, with an eye to improving their health outcomes in the long-term.